Introducing professional advocacy in an acute trust’s X-ray department: a reflective account
Radiographer Adam Prout’s launch of a professional advocacy programme at his trust has helped him support education and quality improvement for staff. Here, he tells Synergy about its progress over the last year




By Adam Prout, senior radiographer
By Adam Prout, senior radiographer
Adam Prout, senior radiographer at Derriford Hospital, has been working to implement professional advocacy in his trust for almost two years now. His own experiences with mental health pushed him to seek new ways to support wellbeing and retention at his trust. After completing a master’s module in professional advocacy in 2024 – becoming at the time one of only two radiographers in the country to have done so – he took to the role with aplomb.
The course enabled him to use ‘emotional interviewing’, a process that supports the individual under supervision to reflect on where they are now and where they want to be. He then works together with them to create an ‘action plan’ on how to get there. Using this process, also known as the ‘A-EQUIP model’, has reduced burnout and stress within the midwifery profession, as well as improving job satisfaction.
Synergy asked Adam about his work within the field, his journey into the role of professional advocate and what changes might be coming in the future.
An idea, a journey, a calling
I first encountered the professional advocacy role through my trust’s neurodiversity staff network. What began as curiosity quickly evolved into something deeper – perhaps an idea, a journey, even a calling.
The Covid pandemic began shortly after I started my first role as a radiographer. Like many early-career professionals, I was navigating a steep learning curve in an already pressured environment. At home, I had a young family; at work, I was stepping into red wards in full PPE, facing the unknown. Toward the end of the pandemic, my mental health deteriorated sharply. I experienced my first panic attack while gowning up for a night shift. Colleagues offered kind words and support, but I brushed them aside – ‘It’s just the children not sleeping’; ‘It’s just Covid.’
What I recognise now is how transformative a structured, confidential and reflective space could have been at that time. That realisation led me to the professional advocacy role and the ‘Advocating for Education and Quality Improvement’ (A-EQUIP) model, developed within NHS England. A-EQUIP provides a person-centred framework that operates outside traditional management hierarchies. It creates space for restorative clinical supervision (RCS), professional development and quality improvement. Crucially, it allows supervisees to bring whatever matters most – workplace challenges, home pressures, career uncertainty – into a psychologically safe conversation.


NHS England
NHS England
This is not therapy. However, evidence from the professional nursing advocate community consistently demonstrates that staff experience RCS as therapeutic in effect. When facilitated effectively, reflective discussion can also be framed through a quality improvement lens, helping colleagues translate reflection into action.
Recent NHS Staff Survey data shows healthcare professionals report increased levels of stress and burnout compared to five years ago, while simultaneously feeling less able to influence change within their organisations. Professional advocacy offers a structured mechanism to address both concerns – supporting wellbeing while enabling meaningful improvement.


Timing, opportunity and implementation
Timing is often everything. As I began exploring how to introduce the role within our acute trust, allied health professionals were being offered access to the associated master’s-level module funded through the NHS England CPD allocation. This created a rare window of opportunity.
One year later, our X-ray department has established a scalable blueprint for implementation. The model is now being rolled out across imaging modalities within our department and has sparked interest across other imaging services and AHP groups within the trust.
Our professional advocacy team is working towards NHS England guidance recommending one professional advocate per 20 healthcare staff, with eight protected hours per month allocated for supervision delivery, including the advocate’s own supervision. While ambitious, these standards provide clarity and direction.
Although supervision is referenced within the 2013 Society of Radiographers supervision guidance and embedded within HCPC Standards of Proficiency (4.8), a local CME session revealed a stark reality: practical application of structured supervision within our X-ray department was effectively zero.
The appetite for change, however, was undeniable. Ninety five per cent of colleagues reported they would benefit from RCS, and 100 per cent agreed the department would benefit from its implementation.
Embedding a culture of reflection and improvement
From the outset, engagement exceeded expectations. Colleagues embraced both the restorative and quality improvement components of A-EQUIP. We deliberately integrated the professional advocacy role into our existing bi-weekly improvement huddles, aligning wellbeing with quality improvement culture.
These huddles have created a structured forum for micro and macro-feedback loops, strengthening engagement and transparency. Linked team health surveys provide both qualitative and quantitative insight into morale. Additionally, linking DATIX submissions into potential RCS ensures appropriate wellbeing and pastoral support is available when incidents occur.
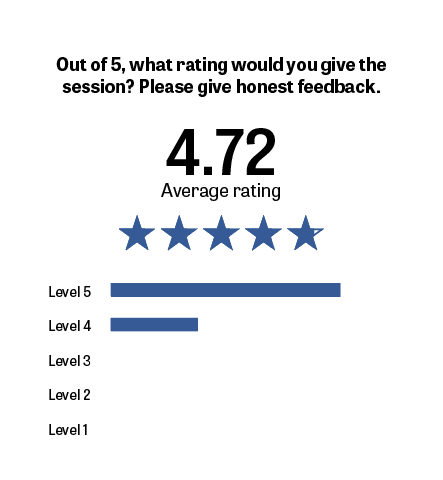
To evaluate impact, we introduced pre and post-session surveys and established four key performance indicators (KPIs):
1. Session satisfaction
Colleagues currently rate sessions at 4.75 out of 5 stars — a strong endorsement of perceived value.

2. Utilisation of protected time
This metric assesses delivery against the recommended protected hours. It consistently sits between 65 and 70 per cent, reflecting the ongoing challenge of balancing supervision with clinical pressures. Research across professional advocacy and supervision literature identifies lack of time and workload intensity as persistent barriers. Our experience mirrors these findings.

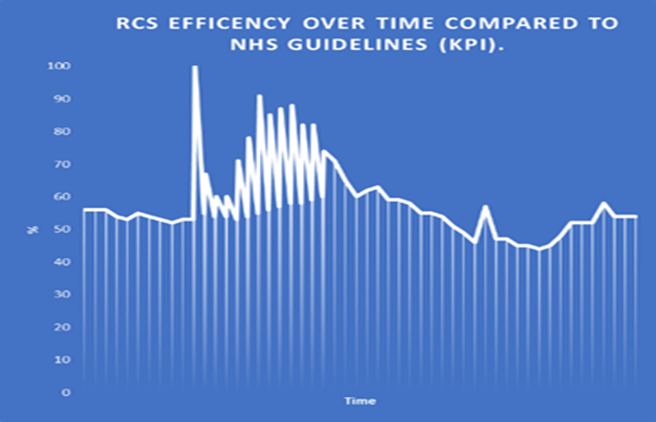
This KPI has taught us our most important lesson: flexibility is essential. Flexibility within the person-centred model – responding to the supervisee’s immediate needs – and flexibility in delivery – adapting to the realities of radiographic workload fluctuations. Any department seeking to replicate this model must recognise that rigid implementation will fail. Scalability is possible, but local politics, staffing pressures and organisational culture must be considered.
3. Number of QI projects
We have developed more than 30 projects during the last calendar year, which has a direct impact on the quality of patient care. Research from the PNA community highlights that the best people to be working within QI are those on the shopfloor. Professional advocacy provides the perfect coaching conditions to maximise this sphere.
4. Team health trends
Data from bi-weekly team health scores provide a longer-term feedback loop, tracking morale and psychological safety over time.

Beyond wellbeing: cultural and financial impact
The influence of professional advocacy extends beyond individual wellbeing. It strengthens psychological safety, retention and engagement – all critical factors in sustainable healthcare delivery.
Quantifying wellbeing improvements is complex. Sickness absence rates and turnover data provide partial indicators, but isolating professional advocacy as the sole causal factor is challenging. However, a supervision policy authored by our trust’s lead professional nursing advocate references Wallbank (2011), whose findings suggest implementation of restorative supervision can reduce mental health-related sickness absence by up to 40 per cent. Trust-level modelling indicates that, across nursing, midwifery and AHP cohorts, such a reduction could equate to approximately £1.34m in savings through reduced sickness absence and bank staffing reliance.
While financial modelling is compelling, the human impact is more profound. Colleagues report feeling better listened to, more empowered to enact change and better able to focus on patient care. Ultimately, patient care remains central to our profession. The ethos underpinning professional advocacy is simple: we cannot care for patients to the best of our ability if we are not also caring for ourselves and each other.


(L-R) Sally Edgington, CEO of AXREM, Rob Emery, regional director at Philips, senior radiographer Adam Prout and Katie Thompson, president of the SoR, presenting Adam with an award for South West Radiography Professional of the Year
(L-R) Sally Edgington, CEO of AXREM, Rob Emery, regional director at Philips, senior radiographer Adam Prout and Katie Thompson, president of the SoR, presenting Adam with an award for South West Radiography Professional of the Year
Recognition and dissemination
The success of our implementation has been reflected in external recognition. I won the 2025 SoR South West Professional Radiographer of the Year award, and we have presented our blueprint at UKIO and across multiple imaging networks and communities of practice.
Feedback from regional and national professional advocates reinforces a shared message: professional advocacy transcends professional boundaries. Its person-centred foundation enables it to address systemic challenges affecting diverse NHS staff groups.
Retention is central to the NHS Long Term Workforce Plan. Supporting staff wellbeing, psychological safety and professional growth cannot be peripheral strategies – they must be embedded within leadership priorities.
We believe professional advocacy should sit at the heart of every healthcare team across the NHS.

Looking forward
Our journey began with personal reflection and a recognition of unmet need. It evolved into a departmental blueprint and is now contributing to wider organisational change.
We do not claim perfection. Clinical pressures remain. Protected time is contested. Cultural transformation is incremental. But the evidence, engagement and outcomes so far suggest that RCS delivered through professional advocacy offers something powerful: a structured, scalable and human framework for supporting staff while improving services.
If our experience can help other departments begin their own journey – adapting the model to local context while embracing flexibility – then our initial spark of curiosity will have been worthwhile.
Professional advocacy is not simply a role. It is a commitment to people, improvement and the principle that caring for our workforce is inseparable from caring for our patients.
Find out more about professional advocacy
Professional advocacy uses the A-EQUIP model, an acronym for advocating for education and quality improvement. The model supports a continuous improvement process that builds personal and professional resilience, enhances quality of care and supports preparedness for appraisal and professional revalidation, with the ultimate goal of making action to improve quality of care an intrinsic part of everyone’s job.
Find out more about the A-EQUIP model online here